
It is always important to be health educated in order not to only understand everything concerning our health condition but even to make the best decision. An example could be one can decide to give birth in the natural way (vaginal) or plan a caesarean procedure. Obviously, such decisions should be discussed with your midwife and /or gynaecologist.
But today, there are definitely two ways of thoughts about it:
- The natural the better!
- I don’t want to feel pain! I prefer the C section!
We have discussed the risk and the recovery after the C section, as for many other surgery procedures. But there is more to understand regarding the C section. First, governments and clinician have observed over the years a rise in numbers of this procedures, with the possible potential of negative consequences for the mother and the infants. Remember that even though with the progress of science and many surgical procedures are safe and very well performed, are not immune to side effects, risks, and complications. But we need even to say that the proportion of caesarean at the population level is a measure of level of access and use of this intervention, and a tool for policy makers and governments in assessing progress in maternal and infant health and emergency obstetric care and resource use.
Another aspect to consider is the cost: a caesarean section represents an expense that not everybody can afford and not every country can guarantee an equitable access to it.
It is reasonable now for you to ask: what should we do?
We are not here to discuss which is the preferable way, but to give you what the literature and the scientific community have stated. Therefore, we present you an extract from the 2015 WHO Statement on Caesarean Section Rates, created after a systematic review of available studies concerning caesarean rates worldwide and the conclusions were:
- Caesarean sections are effective in saving maternal and infant lives, but only when they are required for medically indicated reasons.
- At population level, caesarean section rates higher than 10% are not associated with reductions in maternal and new-born mortality rates.
- Caesarean sections can cause significant and sometimes permanent complications, disability, or death particularly in settings that lack the facilities and/or capacity to properly conduct safe surgery and treat surgical complications. Caesarean sections should ideally only be undertaken when medically necessary.
- Every effort should be made to provide caesarean sections to women in need, rather than striving to achieve a specific rate.
- The effects of caesarean section rates on other outcomes, such as maternal and perinatal morbidity, paediatric outcomes, and psychological or social well-being are still unclear. More research is needed to understand the health effects of caesarean section on immediate and future outcomes.
But to be able to choose if to undergo a c-section, women should be able to decide even where to undergo this procedure. Now there is currently no internationally accepted classification system for caesarean section to compare rates between different facilities, cities, and countries. The only one widely accepted is the 10-group classification (also known as the ‘Robson classification’) that has in recent years become widely used in many countries after the WHO has conducted the systematic review we mentioned above.
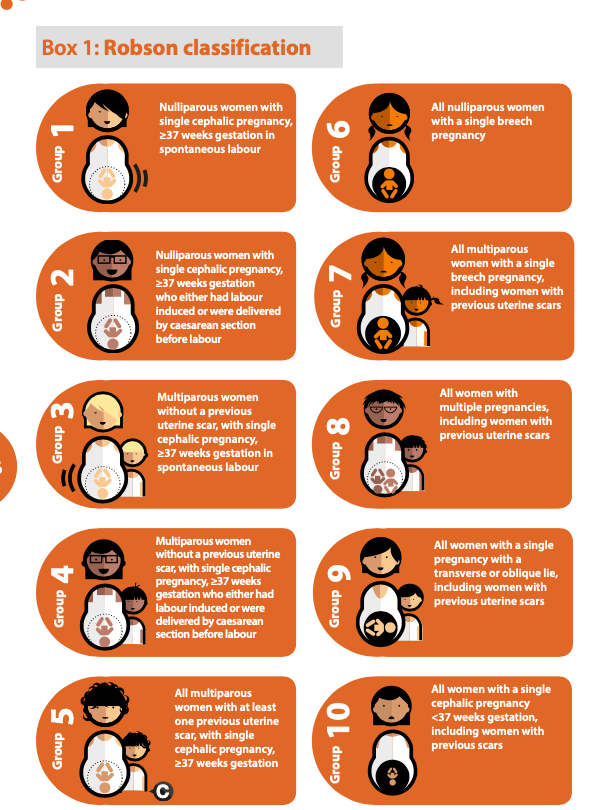
Proposed by Dr Michael Robson in 2001, the classification stratifies women according to their obstetric characteristics, allowing a comparison of caesarean section rates with fewer confounding factors.
So, with this classification, am I able to decide where to get the c-section?
We can’t give a definite answer, considering that the Robinson classification is not exhaustive of all the factors to consider.
But something we can say for sure is that, it is very important to build a trustful relationship with your healthcare providers: our GP, midwife and/or gynaecologist with whom you can discuss all the doubts, the pro, and the cons of this procedure. With all these elements, you will definitely make the correct choice for yourself.
References:
1- WHO Statement on Caesarean Section Rates- World Health Organization 2015
2- Monitoring emergency obstetric care: a handbook. Geneva, Switzerland: World Health Organization, 2009.
3- Victora CG, Barros FC. Beware: unnecessary caesarean sections may be hazardous. Lancet. 2006;367(9525):1796-7.
4- Steer PJ, Modi N. Elective caesarean sections–risks to the infant. Lancet. 2009;374(9691):675-6.
5- Caesarean section–the first cut isn’t the deepest. Lancet. 2010;375(9719):956.
6- Mi J, Liu F. Rate of caesarean section is alarming in China. Lancet. 2014;383(9927):1463-4.
7- Torloni MR, Betran AP, Souza JP, Widmer M, Allen T, Gulmezoglu M, et al. Classifications for cesarean section: a systematic review. PLoS ONE. 2011;6(1):e14566.
8- Betran AP, Vindevoghel N, Souza JP, Gulmezoglu AM, Torloni MR. A Systematic Review of the Robson Classification for Caesarean Section: What Works, Doesn’t Work and How to Improve It. PLoS One. 2014;9(6):e97769.
9- Robson MS. Classification of caesarean sections. Fetal and Maternal Medicine Review. 2001;12(1):23-39.
